
Women face a puzzling dilemma when determining the right time to begin regular breast cancer screenings. Medical organizations offer varying recommendations, with some advocating for screenings to start at 40 or 45 years old, while others recently suggested waiting until age 50. The frequency recommendations also differ, ranging from annual to biennial screenings.
This contradictory guidance exists partly because breast cancer screening recommendations target women with average risk levels who show no cancer symptoms. However, given breast cancer’s prevalence, determining who truly falls into the “average” category and weighing screening benefits against potential drawbacks proves challenging.
“Breast cancer is not one disease,” said Dr. Laura Esserman of the University of California, San Francisco. “So how in the world does it make sense to screen everybody the same when everyone doesn’t have the same risk?”
Dr. Esserman leads research efforts aimed at better identifying women with varying risk levels and ultimately providing more personalized screening recommendations.
According to the American Cancer Society, over 320,000 women in the United States will receive breast cancer diagnoses this year. While mortality rates have declined for decades due to improved treatments, breast cancer remains the second leading cause of cancer-related deaths among American women, and new cases continue to rise slightly.
The American College of Physicians recently issued new recommendations suggesting that women with average risk between ages 50 and 74 receive mammograms every two years. For women aged 40 to 49, the guidelines suggest consulting with physicians about advantages and disadvantages, and if they choose screening, to schedule appointments biennially.
These recommendations, released last month, surprised many in the medical community. Most other American health organizations have encouraged women to begin screenings during their 40s. The U.S. Preventive Services Task Force recently modified its guidance to recommend biennial mammograms starting at 40 rather than 50.
The American Cancer Society has maintained its recommendation for annual mammograms for women aged 45 to 54, though it acknowledges women may choose to begin at 40. For those 55 and older, the organization suggests women can transition to biennial screenings or continue annual examinations.
The American College of Physicians’ new guidelines also suggest physicians may discuss ending routine screenings with women 75 or older. Conversely, the cancer society maintains there’s no need to discontinue screenings for healthy women in this age group.
Women with higher breast cancer risk receive greater benefits from frequent screenings. However, beyond well-established risk factors like BRCA1 or BRCA2 genetic mutations, determining individual risk levels remains difficult. Age serves as a general indicator since breast cancer risk increases with advancing years.
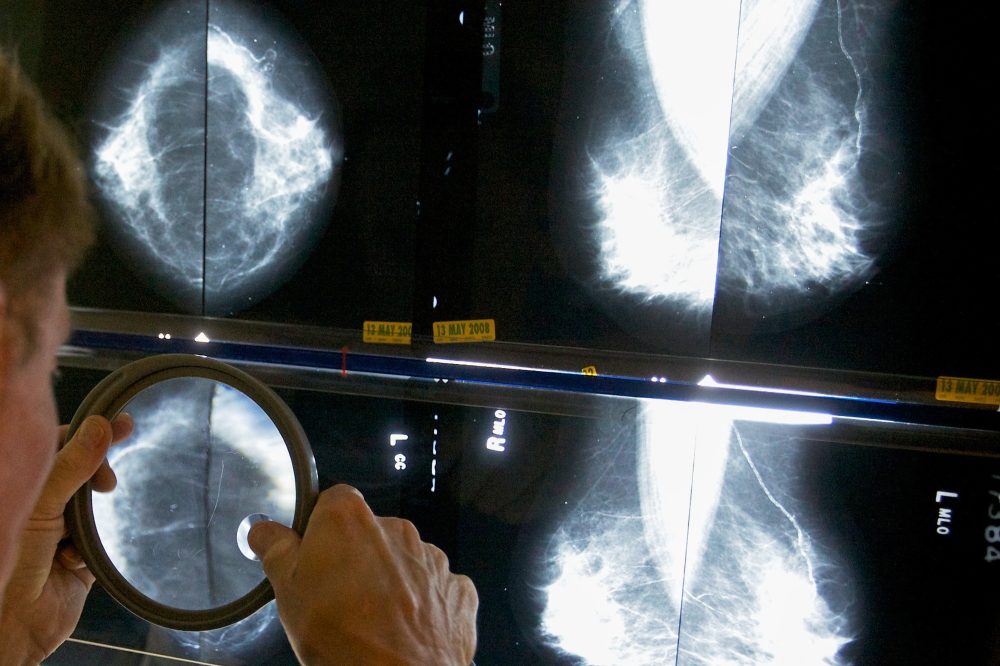
Mammography has limitations, occasionally missing cancers or failing to detect aggressive tumors that develop between routine screenings. Guidelines attempt to balance early cancer detection benefits with potential negative effects, including anxiety and discomfort from investigating suspicious findings that prove benign.
“We’re not saying there’s no benefit” from mammograms in the 40s, cautioned Dr. Carolyn Crandall of the University of California, Los Angeles, who chaired the American College of Physicians report. But “there’s a narrower balance between the benefits you could get and the harms in 40- to 49-year-olds.”
The American Cancer Society supports beginning annual mammograms at 45 after finding breast cancer rates in 45- to 49-year-olds exceeded those in the early 40s, resembling patterns seen in 50- to 54-year-olds, explained public health researcher Robert Smith, the organization’s early cancer detection specialist.
What remains unclear is identifying who might develop aggressive versus slow-growing breast cancers, Smith observed.
Almost half of women over 40 have dense breast tissue, which complicates tumor detection on mammograms and slightly elevates cancer risk.
Women receive breast density notifications following mammograms. Many specialists remain uncertain whether women with dense breasts would benefit from supplemental ultrasounds or MRI screenings. However, the American College of Physicians’ new guidance suggests considering 3D mammography, medically known as digital breast tomosynthesis or DBT.
Future developments may include genetic testing examining factors beyond the well-known BRCA genes, combined with comprehensive risk assessments, to help determine optimal mammogram scheduling for individual women.
A recent study involving nearly 46,000 women, known as the WISDOM trial, utilized age, genetic testing, lifestyle factors, health history, and breast density to categorize participants as low, average, elevated, or high risk. Risk classifications determined whether women delayed screenings until 50, received biennial or annual mammograms, with the highest-risk group undergoing twice-yearly screenings using both mammography and MRI scans. Researchers compared risk-based screening approaches to standard annual mammograms.
Dr. Esserman’s team reported in the medical journal JAMA that risk-based screening performed as effectively as annual screening. One unexpected finding revealed that approximately 30% of women whose genetic testing showed increased risk had no family history of breast cancer. While additional research continues, Dr. Esserman anticipates these preliminary results will begin influencing future guidelines.
Researchers are also developing artificial intelligence tools designed to evaluate women’s short-term breast cancer risk using mammogram data, potentially providing another method for determining appropriate screening frequency.
Currently, women can discuss family cancer history, personal health status, and other risk factors with their physicians, including reproductive history and childbearing age.
Regardless of chosen mammogram timing and frequency, maintaining consistency provides the best outcomes, according to the cancer society’s Smith: “Breast screening works best when it’s done regularly.”